We can STAND BEHIND OUR DIAGNOSTIC DATA
Study designs
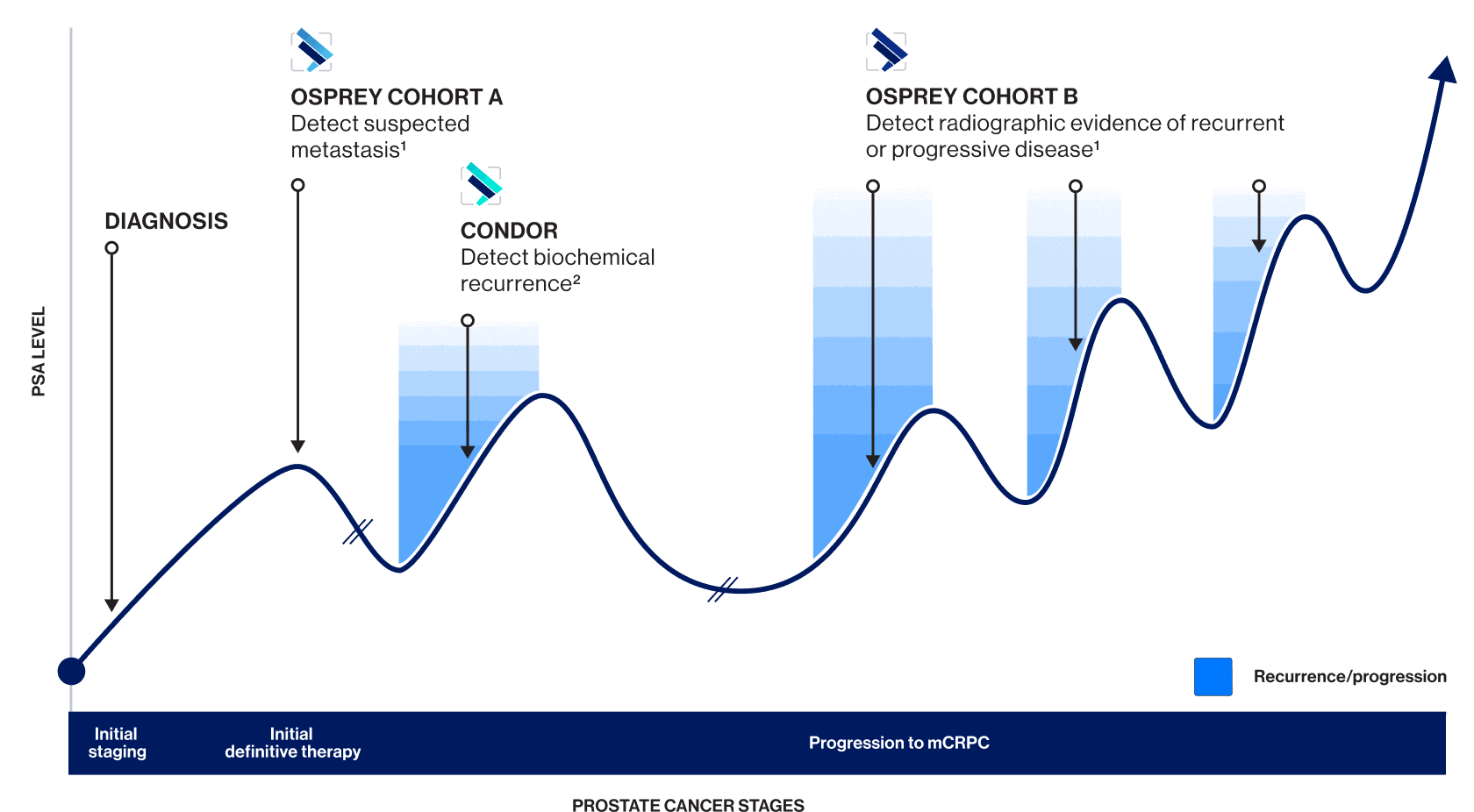
OSPREY COHORT A1
PYLARIFY TruVu: Effectiveness and safety were established based on data from OSPREY—a clinical study of another formulation of piflufolastat F 18
OSPREY was a robust, prospective, multicenter, phase 2/3 clinical trial of 385 patients. In Cohort A, 268 men with high-risk prostate cancer had evaluable histopathology for determining the diagnostic performance of the imaging agent in identifying pelvic nodal metastases.
OSPREY Cohort A assessed sensitivity, specificity, PPV, and NPV in pelvic lymph nodes and in the prostate gland for PSMA-targeted PET.
Patient population
Men with high-risk PCa (clinical stage ≥T3a, PSA >20 ng/mL, or Gleason score ≥8 with planned RP-PLND).
Patients with prior androgen deprivation therapy or any investigational neoadjuvant agent or intervention were excluded1,2
PSMA-targeted PET
9 mCi (333 MBq) IV, followed by PET/CT after 1-2 hours
Evaluation
252 men underwent surgery and had PLND evaluated locally by pathologists blinded to the imaging result. 16 men did not undergo RP-PLND. All scans were submitted for central imaging reviewed by 3 blinded independent board-certified nuclear medicine specialists
Co-primary endpoints:
- Specificity
- Sensitivity
Secondary endpoints:
- PPV
- NPV
- Detection of primary tumor within the prostate
- Detection of M1 disease
In Cohort A, OSPREY included high-risk patients across a range of PSA levels, disease stages, age ranges, and Gleason scores*
*n=268; except for Distant Metastases (n=266) and Median PSA (n=267).
†Stage at time of study entry or most recent prior to entry.
AJCC=American Joint Commission on Cancer; NPV=negative predictive value; PCa=prostate cancer; PET=positron emission tomography; PLND=pelvic lymph node dissection; PPV=positive predictive value; PSA=prostate-specific antigen; RP-PLND=radical prostatectomy and pelvic lymph node dissection.
CONDOR3
PYLARIFY TruVu: Effectiveness and safety were established based on data from CONDOR—a clinical study of another formulation of piflufolastat F 18
CONDOR was a robust, multicenter, phase 3 trial of 208 patients with suspected recurrent or metastatic prostate cancer with negative or equivocal results using standard imaging. CONDOR assessed correct localization rate (CLR)—an improved metric for evaluating diagnostic performance compared to PPV—in patients with biochemically recurrent prostate cancer.*
*CLR is defined as positive predictive value with an additional requirement of anatomic lesion colocalization with a composite standard of truth.
Patient population
Men with biochemically recurrent prostate cancer previously treated with radical prostatectomy and/or radiation therapy. All patients had negative/equivocal findings for prostate cancer on standard imaging 60 days before receiving PSMA PET
Exclusion criteria included administration of any high-energy (>300 KeV) gamma-emitting radioisotope within 5 physical half-lives prior to injection, androgen deprivation therapy (ADT) within 3 months of imaging, investigational therapy for prostate cancer within 60 days of imaging, and ongoing systemic therapy
PSMA-targeted PET
A single dose of 9 mCi (333 MBq) IV 1-2 hours before PET/CT
Evaluation
208 men underwent scan. Assessment was performed by 3 independent, blinded, board-certified nuclear medicine physicians. Patients with positive scans were scheduled for follow-up to verify suspected lesions based on composite standard of truth (SOT)
Primary endpoint:
- CLR
Secondary endpoint:
- Percentage of patients with a change in intended treatment plan based on pre- and post-medical management questionnaires (MMQs) completed by treating investigators. MMQs were available for 205 out of 208 patients
For patients treated with RP, BCR was defined as PSA rising to ≥0.2 ng/mL
For patients treated with RT, BCR was defined as a PSA value ≥2 ng/mL above the patient’s post-radiation nadir value
Reference standards of truth in CONDOR
Because most patients were not expected to have an amenable lesion for histological verification, a composite standard of truth was agreed to with the FDA based on these reference standards (in order of priority):
Evaluable histopathology results from prostatectomy, salvage pelvic lymph node dissection, or targeted biopsy
Correlative follow-up imaging findings using F 18 fluciclovine or 11 C choline PET, or focused MRI or CT
If neither of the above was available or informative, confirmed PSA response† up to 9 months post-radiation initiation (without concomitant ADT) of all PET-positive foci
†PSA response was defined as PSA decline by >50% from baseline that was confirmed on repeat measurement within 4 weeks, based on central laboratory results.
CONDOR included BCR patients with a broad range of PSA levels and Gleason scores ranging from 6-9
ADT=androgen deprivation therapy; BCR=biochemical recurrence; CLR=correct localization rate; CT=computed tomography; FDA=US Food and Drug Administration; MBq=megabecquerel; mCi=millicurie; MRI=magnetic resonance imaging; PCa=prostate cancer; PET=positron emission tomography; PPV=positive predictive value; PSA=prostate-specific antigen; PSMA=prostate-specific membrane antigen; RP=radical prostatectomy; RT=radiation therapy; SOT=standard of truth.
OSPREY COHORT B1
PYLARIFY TruVu: Effectiveness and safety were established based on data from OSPREY—a clinical study of another formulation of piflufolastat F 18
OSPREY was a robust, prospective, multicenter, phase 2/3 clinical trial of 385 patients. OSPREY Cohort B assessed sensitivity and PPV in 117 patients with radiologic evidence of recurrence.
Patient population
Men with radiologic evidence of recurrence
Exclusion criteria included prior radiation or ablative therapy to intended site biopsy if within the prostate bed and initiation of new therapy for recurrent and/or progressive metastatic disease since radiographic documentation of recurrence/progression
Baseline conventional imaging
CT, MRI, or bone scan 4-6 weeks before PSMA PET
PSMA-targeted PET
9 mCi (333 MBq) IV, followed by PET/CT after 1-2 hours
Evaluation
Lesions (biopsy) detected by CT, MRI, or bone scan, evaluated for presence or absence of PCa or other neoplasm, or deemed unevaluable
Formal hypothesis testing was not employed for Cohort B endpoints
Secondary endpoints:
- Sensitivity*
- PPV
*With subanalyses by region and PSA level.
CT=computed tomography; MRI=magnetic resonance imaging; PCa=prostate cancer; PET=positron emission tomography; PPV=positive predictive value.
INDICATION
PYLARIFY TRUVU (piflufolastat F 18) Injection is indicated for positron emission tomography (PET) of prostate-specific membrane antigen (PSMA) positive lesions in men with prostate cancer:
- with suspected metastasis who are candidates for initial definitive therapy.
- with suspected recurrence based on elevated serum prostate-specific antigen (PSA) level.
IMPORTANT SAFETY INFORMATION
Warnings and Precautions
Risk of Image Misinterpretation
Imaging interpretation errors can occur with PYLARIFY TRUVU imaging. A negative image does not rule out the presence of prostate cancer and a positive image does not confirm the presence of prostate cancer. The performance of PYLARIFY TRUVU for imaging biochemical evidence of recurrence of prostate cancer seems to be affected by serum PSA levels. The performance of PYLARIFY TRUVU for imaging of metastatic pelvic lymph nodes prior to initial definitive therapy seems to be affected by risk factors such as Gleason score and tumor stage. PYLARIFY TRUVU uptake is not specific for prostate cancer and may occur with other types of cancer as well as non-malignant processes and in normal tissues. Clinical correlation, which may include histopathological evaluation, is recommended.
Hypersensitivity Reactions
Monitor patients for hypersensitivity reactions, particularly those with a history of allergy to other drugs and foods. Reactions may be delayed. Always have trained staff and resuscitation equipment available.
Radiation Risks
PYLARIFY TRUVU exposes patients to radiation. Radiation exposure is associated with a dose-dependent increased risk of cancer. Ensure safe handling and preparation procedures to protect patients and health care workers from unintentional radiation exposure. Advise patients to hydrate before and after administration and to void frequently after administration.
Adverse Reactions
The most frequently reported adverse reactions were headaches, dysgeusia and fatigue, occurring at rate of ≤2% during clinical studies. In addition, a delayed hypersensitivity reaction was reported in one patient (0.2%) with a history of allergic reactions.
Drug Interactions
Androgen deprivation therapy (ADT) and other therapies targeting the androgen pathway, such as androgen receptor antagonists, may result in changes in uptake of PYLARIFY TRUVU in prostate cancer. The effect of these therapies on performance of PYLARIFY TRUVU PET has not been established.
REFERENCES
1. Pienta KJ, Gorin MA, Rowe SP, et al. A phase 2/3 prospective multicenter study of the diagnostic accuracy of prostate specific membrane antigen PET/CT with 18F-DCFPyL in prostate cancer patients (OSPREY). J Urol. 2021;206(1):52-61. 2. ClinicalTrials.gov. Study NCT02981368: Study of 18F-DCFPyL PET/CT imaging in patients with prostate cancer (OSPREY). Accessed April 21, 2026. https://clinicaltrials.gov/study/NCT02981368 3. Morris MJ, Rowe SP, Gorin MA, et al. Diagnostic performance of 18F-DCFPyL-PET/CT in men with biochemically recurrent prostate cancer: results from the CONDOR phase III, multicenter study. Clin Cancer Res. 2021;27(13):3674-3682.