We can deliver diagnostic precision
Study results
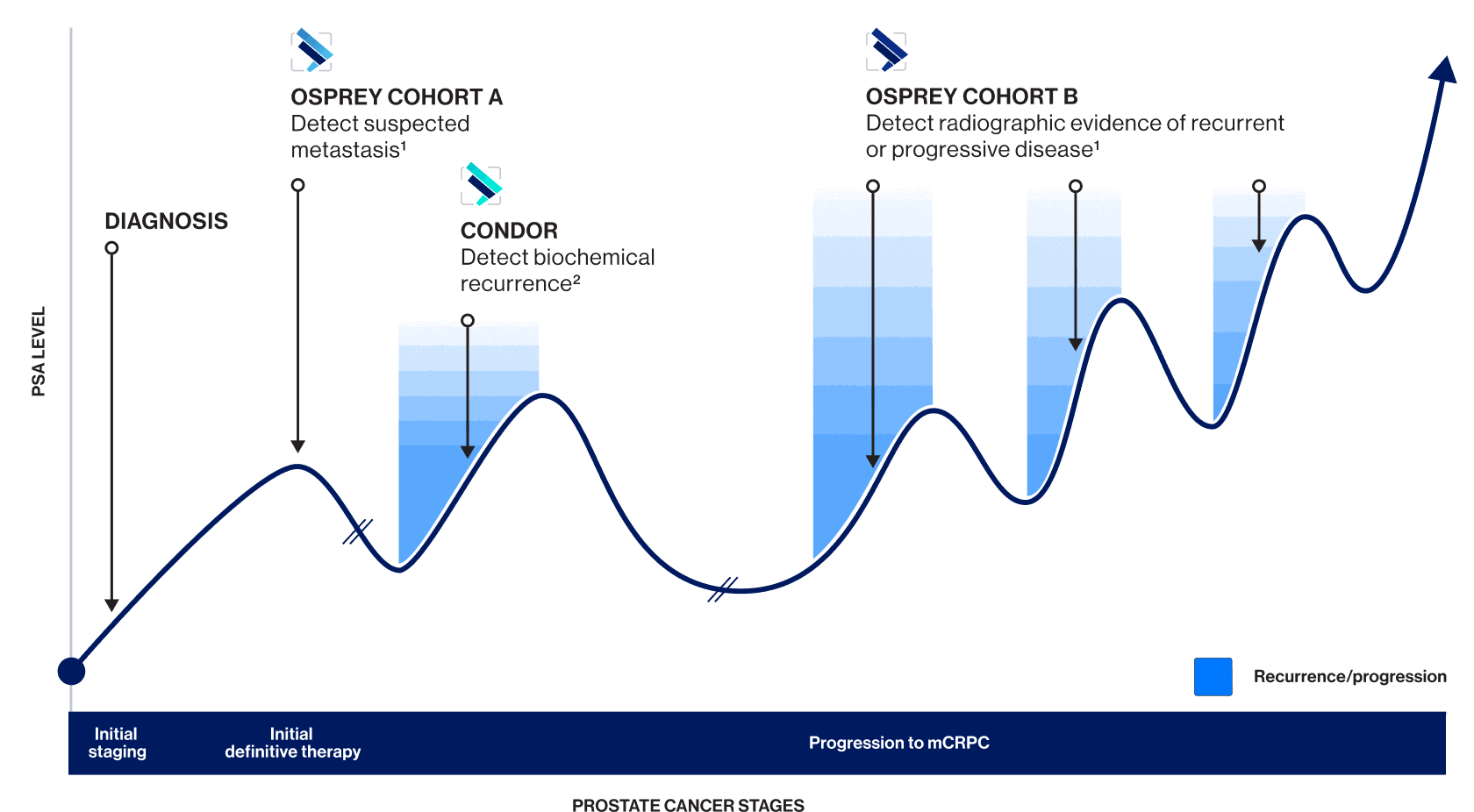
OSPREY Cohort A
PYLARIFY TruVu: Effectiveness and safety at initial staging were established based on data from OSPREY Cohort A—a clinical study of another formulation of piflufolastat F 18
Clarity at initial staging
Pre-specified analysis and post-hoc analysis1
In the pre-specified analysis, the specificity co-primary endpoint was met (the lower limits of the 95% CIs for all readers were >80%), but the sensitivity co-primary endpoint was not met.
Post-hoc analysis was conducted evaluating PET/CT for detection of nodal metastases >5 mm. 27 patients were excluded whose largest nodal metastasis was ≤5 mm.
Co-primary endpoints:
- Specificity: 96% median (endpoint met — lower limits of 95% CIs for all readers exceeding pre-specified 80% threshold)
- Sensitivity: 38% median (endpoint not met)
Compared to standard imaging, PSMA-targeted PET scan with piflufolastat F 18 delivered3:
Higher specificity
(96.3%–98.9% vs 65.1%)
Nearly 3 times the PPV
(78.1%–90.5% vs 28.3%)
Similar sensitivity to standard imaging
(30.6%–41.9% vs 42.6%)
This clinical study demonstrated accurate lesion detection vs conventional imaging for high-risk patients1
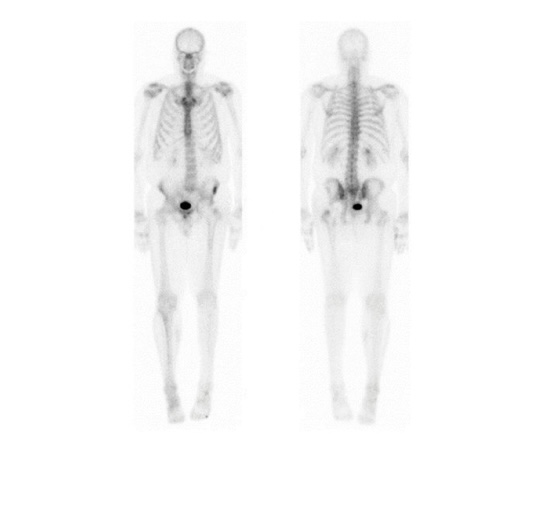 Anterior
Posterior
Anterior
Posterior
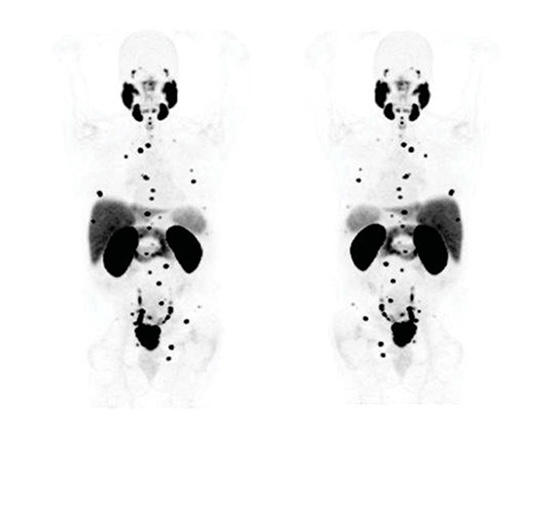 Anterior
Posterior
Anterior
Posterior
Adapted from Pienta K, Gorin M, Rowe S, et al. A phase 2/3 prospective multicenter study of the diagnostic accuracy of prostate specific membrane antigen PET/CT with 18F-DCFPyL in prostate cancer patients (OSPREY). J Urol. 2021;206(1):52-61.
In OSPREY Cohort A, reader agreement was substantial to almost perfect across all 3 readers3:
Substantial intra-reader agreement
(0.78 Fleiss kappa)
Moderate to almost perfect intra-reader agreement
(0.79–1.0 Cohen’s kappa)
Substantial agreement=Fleiss kappa of 0.61-0.80; moderate to almost perfect intra-reader agreement=Cohen’s kappa of 0.60-0.79+.4,5
CI=confidence interval; NPV=negative predictive value; PET=positron emission tomography; PPV=positive predictive value; PSMA=prostate-specific membrane antigen.
CONDOR
PYLARIFY TruVu: Effectiveness and safety in BCR were established based on data from CONDOR—a clinical study of another formulation of piflufolastat F 18
Clarity upon recurrence
Correct localization rate (CLR) validates precision6
CLR is a unique endpoint that confirms lesions and pinpoints their precise location. This precision can help inform treatment decisions for your patients.

Why trust CLR?
CLR at the patient level is the percentage of patients with a one-to-one correspondence between lesion level of ≥1 lesion on PSMA PET imaging and the standard of truth.6
CLR equates to PPV (TP/TP+FP) with the added requirement of precise anatomic location matching.6
| PSMA PET central reader findings | Standard of Truth findings | PPV | CLR | Result |
|---|---|---|---|---|
| Right common iliac LN | Right common iliac LN | 100% | 100% | Anatomic match |
| Left pelvic bone | Right pelvic bone | 100% | 0 | Anatomic mismatch |
High CLR: Surpassed Primary Endpoint Threshold in All Readers*
These results significantly exceeded the predetermined threshold of 20% in the CONDOR study, for all 3 readers2,6
*CLR was assessed against a composite standard of truth that included histopathology, correlative imaging and or PSA response following directed therapy, as applicable.
†The lower bound of the 95% CI ranged from 77.8%-80.4%.
In the CONDOR study, the detection rate rose with increasing PSA levels6
CLR at all evaluated PSA levels6
We can deliver
consistent clarity
High true positives with low false positives provide additional confirmation of accuracy in BCR, enabling physicians to make treatment choices with confidence. In contrast, high false positives may throw off accurate assessment of the presence and extent of prostate cancer, risking overtreatment.6
86%
True Positives‡
14%
False Positives‡
‡Median result of 3 independent readers, 95% CI (78.8-92.3).
In CONDOR, reader agreement was substantial to almost perfect7§
Substantial inter-reader agreement
(0.65 Fleiss kappa)
Strong to almost perfect intra-reader agreement
(0.81–1.0 Cohen’s kappa)
§Substantial agreement=Fleiss kappa of 0.61-0.80; strong to almost perfect intra-reader agreement=Cohen’s kappa of 0.80-1.0.4,5
BCR=biochemical recurrence; CLR=correct localization rate; FP=false positive; LN=lymph node; PET=positron emission tomography; PPV=positive predictive value; PSMA=prostate-specific membrane antigen; TP=true positive.
OSPREY Cohort B
Region-level PPV
The OSPREY Cohort B presented region-level PPV of 81%–90% in men with radiographic recurrence across all measured sites of disease metastasis, including bone1
In Cohort B (93 evaluable patients, median PSA 11.3 ng/mL), median sensitivity and positive predictive value for extraprostatic lesions were 95.8% (87.8%–99.0%) and 81.9% (73.7%–90.2%) respectively.
High sensitivity across regions ensures a low false-negative rate
Formal hypothesis testing was not employed for Cohort B. Results are descriptive; no definitive conclusions can be made.
PPV=positive predictive value; PSA=prostate-specific antigen.
INDICATION
PYLARIFY TRUVU (piflufolastat F 18) Injection is indicated for positron emission tomography (PET) of prostate-specific membrane antigen (PSMA) positive lesions in men with prostate cancer:
- with suspected metastasis who are candidates for initial definitive therapy.
- with suspected recurrence based on elevated serum prostate-specific antigen (PSA) level.
IMPORTANT SAFETY INFORMATION
Warnings and Precautions
Risk of Image Misinterpretation
Imaging interpretation errors can occur with PYLARIFY TRUVU imaging. A negative image does not rule out the presence of prostate cancer and a positive image does not confirm the presence of prostate cancer. The performance of PYLARIFY TRUVU for imaging biochemical evidence of recurrence of prostate cancer seems to be affected by serum PSA levels. The performance of PYLARIFY TRUVU for imaging of metastatic pelvic lymph nodes prior to initial definitive therapy seems to be affected by risk factors such as Gleason score and tumor stage. PYLARIFY TRUVU uptake is not specific for prostate cancer and may occur with other types of cancer as well as non-malignant processes and in normal tissues. Clinical correlation, which may include histopathological evaluation, is recommended.
Hypersensitivity Reactions
Monitor patients for hypersensitivity reactions, particularly those with a history of allergy to other drugs and foods. Reactions may be delayed. Always have trained staff and resuscitation equipment available.
Radiation Risks
PYLARIFY TRUVU exposes patients to radiation. Radiation exposure is associated with a dose-dependent increased risk of cancer. Ensure safe handling and preparation procedures to protect patients and health care workers from unintentional radiation exposure. Advise patients to hydrate before and after administration and to void frequently after administration.
Adverse Reactions
The most frequently reported adverse reactions were headaches, dysgeusia and fatigue, occurring at rate of ≤2% during clinical studies. In addition, a delayed hypersensitivity reaction was reported in one patient (0.2%) with a history of allergic reactions.
Drug Interactions
Androgen deprivation therapy (ADT) and other therapies targeting the androgen pathway, such as androgen receptor antagonists, may result in changes in uptake of PYLARIFY TRUVU in prostate cancer. The effect of these therapies on performance of PYLARIFY TRUVU PET has not been established.
REFERENCES
1. Pienta KJ, Gorin MA, Rowe SP, et al. A phase 2/3 prospective multicenter study of the diagnostic accuracy of prostate specific membrane antigen PET/CT with 18F-DCFPyL in prostate cancer patients (OSPREY). J Urol. 2021;206(1):52-61. 2. PYLARIFY TruVu™ [package insert]. North Billerica, MA: Aphelion LLC, a Lantheus company. 3. Pienta KJ, Gorin MA, Rowe SP, et al. A phase 2/3 prospective multicenter study of the diagnostic accuracy of prostate specific membrane antigen PET/CT with 18F-DCFPyL in prostate cancer patients (OSPREY). Supplementary Appendix. J Urol. 2021;206(1):52-61. 4. Sreedhara VSM, Mocko G. Control of thermoforming process parameters to increase quality of surfaces using pin-based tooling. Proceedings of the ASME 2015 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference. Boston, MA, USA. August 2-5. V004T05A016. 5. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276-282. 6. Morris MJ, Rowe SP, Gorin MA, et al. Diagnostic performance of 18F-DCFPyL-PET/CT in men with biochemically recurrent prostate cancer: results from the CONDOR phase III, multicenter study. Clin Cancer Res. 2021;27(13):3674-3682. 7. Morris MJ, Rowe SP, Gorin MA, et al. Diagnostic performance of 18F-DCFPyL-PET/CT in men with biochemically recurrent prostate cancer: results from the CONDOR phase III, multicenter study. Supplementary Appendix. Clin Cancer Res. 2021;27(13):3674-3682.